Despite US drug overdose deaths declining from 2022 to 2025, the supply of illegal drugs is unpredictable. Illicitly manufactured fentanyl is involved in many deaths and is frequently mixed with other drugs such as benzodiazepines or xylazine. Meditomidine, an alpha-2 adrenergic agonist sedative, more potent and longer-acting than clonidine and xylazine, was first identified in the illicit drug supply in 2021 and began appearing coincidentally with fentanyl in several jurisdictions, including Chicago.Philadelphiaand Pittsburgh From mid-2023 to mid-2024. As of late July 2024, methotrexate was detected in drug samples and biological samples from people who used illegal opioids in at least 18 states and the District of Columbia..
The geographic distribution of meditomidine appears to be expanding; Number of reports submitted to the National Forensic Laboratory Information System (NFLIS).which obtains forensic laboratory findings from law enforcement drug seizures, increased 950% from 247 in 2023 to 2,616 in 2024, followed by a 215% increase to 8,233 in 2025. Reports of medetomidine included.
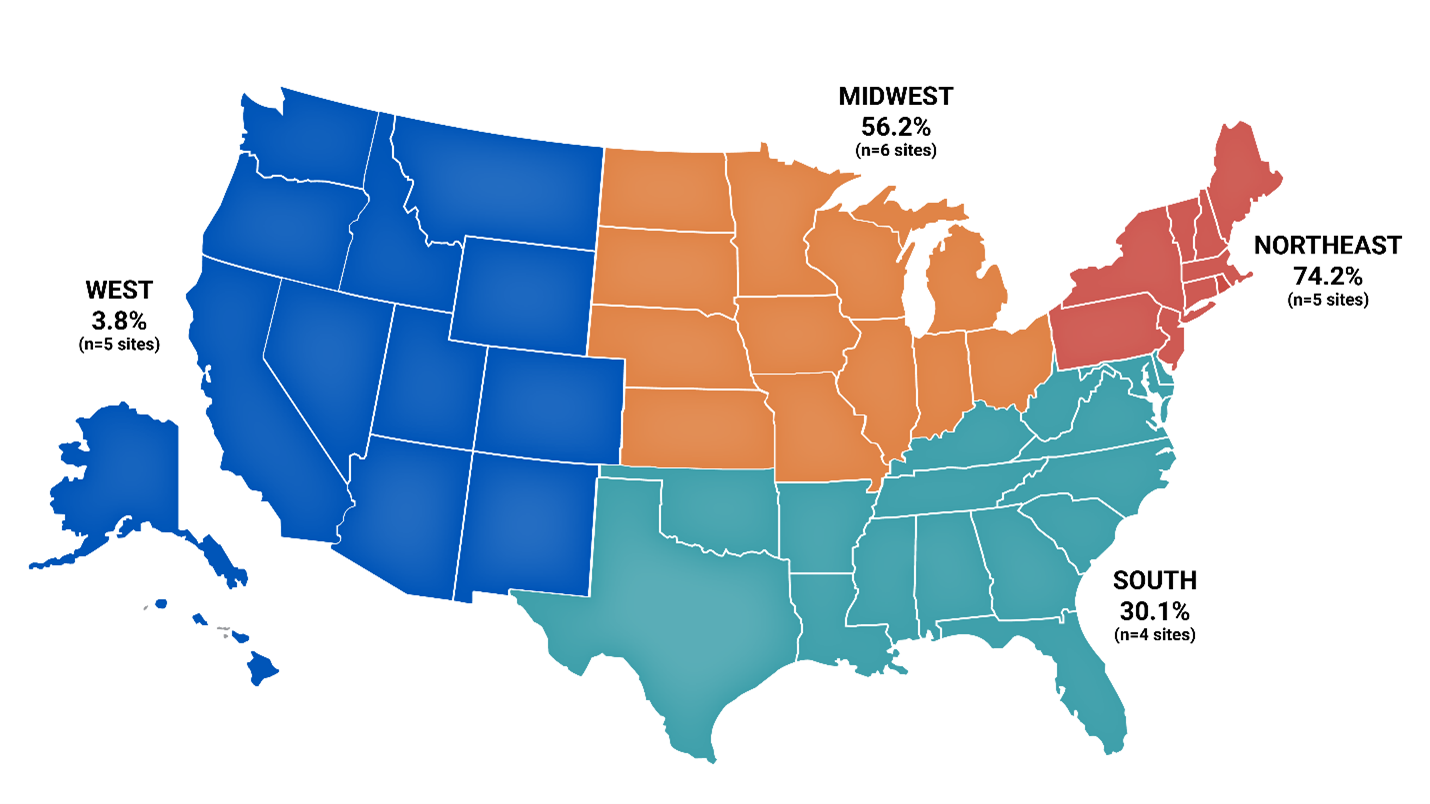
From October 2025 to January 2026, medetomidine was detected weekly in treated wastewater in at least 14 states enrolled in a wastewater testing program in the United States. Data from the CDC’s Overdose Data Action (OD2A) program, which funds local health departments to conduct laboratory testing of drug products and paraphernalia, and the National Institute of Standards and Technology’s (NIST) radar programfound that 10 of 20 sentinel sites detected medetomidine in nearly 35% of opioid-positive samples from July 2025-December 2025 (Figure). These sites were most often located in northeastern states (n = 5 of 5 sites), followed by Midwestern states (n = 4 of 6 sites), and southern states (n = 1 of 4 sites). All five sites in the western states detected medetomidine in their opioid-positive samples, but at low levels, ranging from 2% to 8%. Eight sites detected medetomidine in more than 50% of opioid-positive samples. Among pharmaceutical product samples (eg, powders or pills) with positive test results for medetomidine (n=995) from July 2025 to December 2025, 98% were detected with fentanyl, with medetomidine reportedly mixed with products sold as fentanyl, as noted in local advertisements.
Figure: Percentage of opioid-positive drug product and paraphernalia samples positive for medetomidine at 20 sentinel sitesa: United States region, July 2025 – December 2025 (provisional data)b, c
a. The 20 sites include the Midwest (Chicago Public Health Department, IL; Cuyahoga County Board of Health, OH; Hamilton County Public Health, OH; Health and Hospital Corporation of Marion County, IN; St. Fund for Public Health, PA, PA; [Philadelphia, PA] In collaboration with Partners Research Institute, South (Florida Department of Health – Broward County, FL; Delaware Department of Health and Human Services; Maryland Department of Health; Florida Department of Health – Palm Beach County, FL), West (Alameda County Health Care Services Agency, CA; Denver County and Department of Public Health, Angell County, Department of Public Health, Angell County Public Health, CA; Public Health – Seattle and King County, Southern Nevada Health District, NV).
b. The total number of samples tested per site ranged from 102 to 1,216 (median = 308) and was a convenience sample. Thus, overall percentages do not represent local or regional drug use.
c. The types of samples (eg, drug products, drug paraphernalia) tested varied across sites. Thus, the presence of drugs in the drug market is overestimated because drug paraphernalia may be used multiple times by many people and drug samples may be contaminated in trace amounts due to storage or handling.
Reported side effects of methotrexate are consistent with those of alpha-2 agonists and include:
- Marked bradycardia (heart rate as low as 32 beats per minute)
- Hypertension, and
- Deep, often prolonged rest.
Unlike xylazine, medetomidine use is not associated with the development of ulcers.
Because fentanyl is involved in large amounts of medetomidine, OORMs should be administered in suspected doses to restore normal breathing. OORMs such as naloxone are effective in reversing the effects of opioids but are not effective in reversing the effects of medetomidine or other drugs that may have been consumed. Consequently, while apnea may be reversible with naloxone, sedation may not be. Frequency of respiratory support and intensive care unit (ICU) management for overdoses involving medetomidine compared with opioid or stimulant overdoses without medetomidine, regardless of withdrawal symptoms..
The occurrence of medetomidine in illicit opioid supplies has been associated with overdose clusters, including 12 confirmed, 26 probable, and 140 suspected medetomidine overdoses in Chicago in May 2024; Fentanyl was detected in all medetomidine positive samples. Most patients present with opioid dose-specific findings and co-opioid involvement (altered mental status, pupillary signs, hypoxemia). Most had significant bradycardia due to the alpha agonist effect of medetomidine, some requiring atropine. At least 16 people were hospitalized and one died.
Stopping meditomidine after regular use can cause a severe withdrawal syndrome, similar to clonidine withdrawal, that requires emergency or intensive care. Symptoms of withdrawal include:
- Tachycardia (>100 beats per minute)
- severe hypertension,
- change notice,
- shock
- Chest pain, and
- Nausea and vomiting.
Withdrawal symptoms may begin within hours of last use and peak 18-36 hours later. Complications such as non-ST-elevation myocardial infarction and posterior reversible encephalopathy syndrome have been associated with acute withdrawal of medetomidine. Increases in emergency department visits for non-alcohol, non-nicotine, and non-cannabis withdrawal have been temporally associated with the discovery of medetomidine in the drug supply, with continued prevalence associated with significant emergency department and ICU utilization. From September 2024 to January 2025, 165 patients at three Philadelphia health systems were hospitalized for fentanyl withdrawal complicated by severe autonomic dysfunction. Similar presentations were reported in Pittsburgh (October 2024–March 2025), where many patients required dexmedetomidine infusions and ICU-level care, and in Maryland (July 2025–August 2025), where medetomidine-related overdoses were frequent withdrawal symptoms.
CDC helps states and local communities detect, prevent, and respond to health threats through ongoing technical assistance and support through CDC’s Overdose Data Action (OD2A) Collaborative Agreement and the Overdose Response Strategy (ORS).. ONDCP Develops a national drug control strategy to coordinate government efforts to reduce the supply and demand for illicit drugs, and to track and communicate about growing and emerging threats.
#Illegal #fentanyl #supply #United #States #increases #risk #overdose #acute #withdrawal #syndrome